What is Sickle Cell Disease?
Avascular Necrosis in Sickle Cell is one of the most serious orthopedic complications of Sickle Cell Disease (SCD). Sickle Cell Disease is an inherited blood disorder in which red blood cells become hard, sticky, and crescent (sickle) shaped instead of their normal round shape. These abnormal cells can block small blood vessels, reducing blood flow and oxygen delivery to different parts of the body, especially the bones.
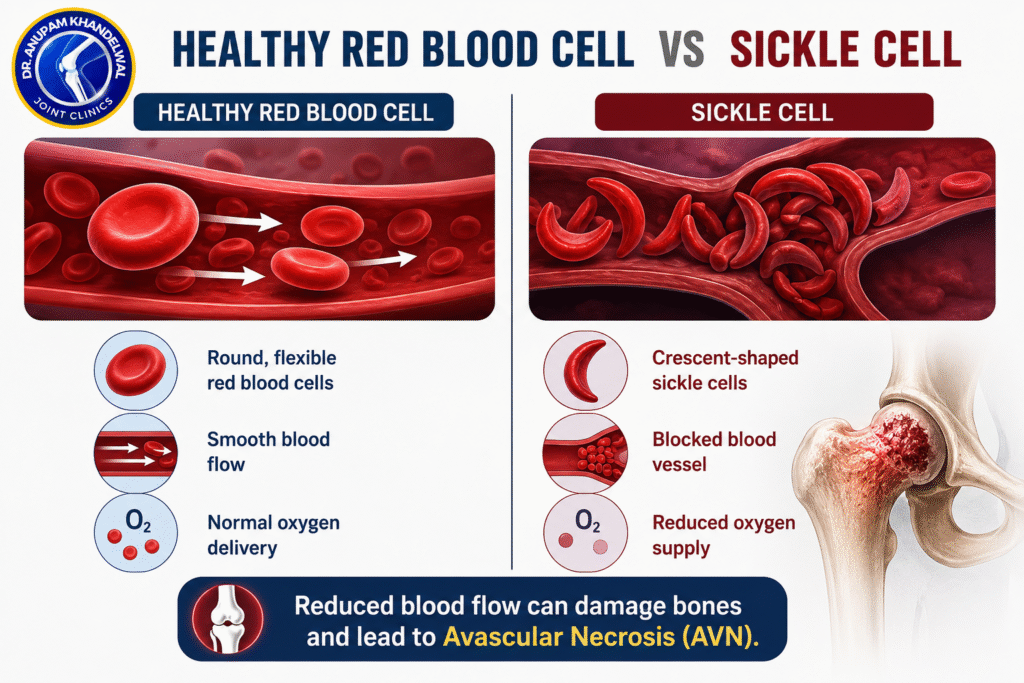
Healthy red blood cells are round, flexible, and move easily through tiny blood vessels to supply oxygen and nutrients to tissues. In contrast, sickle-shaped red blood cells become rigid and can get trapped inside narrow blood vessels, interrupting normal circulation. Repeated blockage of blood flow prevents the bones from receiving enough oxygen, particularly in the hip joint.
Over time, the lack of blood supply causes bone tissue to die, leading to Avascular Necrosis in Sickle Cell. If left untreated, this condition can weaken the femoral head, cause bone collapse, lead to severe hip arthritis, and eventually require hip replacement surgery. Early diagnosis and timely treatment are essential to preserve the natural hip joint and improve long-term mobility.
Normal Red Blood Cell vs Sickle Cell
Because of these repeated blockages, bones—especially the hip joint—receive less oxygen and nutrients, increasing the risk of Avascular Necrosis in Sickle Cell.
What is Avascular Necrosis in Sickle Cell?
Avascular Necrosis (AVN), also called osteonecrosis, is a condition in which bone tissue dies because it no longer receives enough blood supply.
The femoral head (the ball-shaped upper end of the thigh bone) is particularly vulnerable because it depends on a delicate network of blood vessels. Once these vessels become blocked, the bone gradually weakens and collapses.
Without timely treatment, AVN can destroy the hip joint and eventually require total hip replacement surgery.
Why Does Avascular Necrosis Occur in Sickle Cell Disease?
Avascular Necrosis in Sickle Cell develops because sickle-shaped blood cells repeatedly obstruct the tiny arteries that supply blood to bones.
The process typically occurs as follows:
- Sickle cells block small blood vessels.
- Blood flow to the femoral head decreases.
- Bone cells receive less oxygen.
- Bone tissue begins to die.
- Small fractures develop inside the bone.
- The femoral head loses its shape.
- Hip arthritis develops over time.
Patients with frequent sickle cell crises have a higher risk of developing AVN.
Which Bones Are Commonly Affected?
Although AVN can occur in many bones, the most commonly affected areas include:
- Hip (Femoral Head)
- Shoulder
- Knee
- Ankle
- Wrist
The hip is involved in nearly 80–90% of symptomatic cases.
How Common is Avascular Necrosis in Sickle Cell?
Studies suggest that between 10% and 50% of patients with sickle cell disease may develop AVN during their lifetime, depending on the severity of their disease and age.
Many patients develop AVN in both hips, making early diagnosis especially important.
What is a Sickle Cell Crisis?
A Sickle Cell Crisis, also called a pain crisis or vaso-occlusive crisis, is a painful episode that occurs when sickle-shaped red blood cells block small blood vessels. This reduces the blood supply to different parts of the body, causing severe pain and tissue damage.
Patients may experience:
- Sudden severe pain in the bones or joints
- Hip, shoulder, back, chest, or leg pain
- Swelling in the affected area
- Difficulty walking if the hip joint is involved
- Fever or tiredness in some cases
Repeated pain crises can reduce the blood supply to the hip joint over time. In some patients, this may contribute to the development of Avascular Necrosis (AVN), where the bone tissue begins to die because it is not receiving enough blood.
If a pain crisis is severe, lasts longer than usual, or is associated with fever, breathing difficulty, or an inability to walk, medical attention should be sought promptly.
Types of Sickle Cell Crisis
1. Vaso-Occlusive Crisis (Pain Crisis)
This is the most common type of sickle cell crisis. Sickle-shaped red blood cells block small blood vessels, reducing blood flow to tissues. Patients experience sudden, severe pain, usually in the bones, joints, hips, back, arms, or legs. Repeated vaso-occlusive crises can contribute to reduced blood supply to the hip, increasing the risk of Avascular Necrosis (AVN).
2. Aplastic Crisis
This occurs when the bone marrow temporarily stops producing enough red blood cells, often due to an infection such as Parvovirus B19. Patients may develop severe anemia, weakness, dizziness, and fatigue. Immediate medical evaluation is usually required.
3. Splenic Sequestration Crisis
In this condition, a large amount of blood suddenly becomes trapped in the spleen, causing the spleen to enlarge rapidly and leading to a sudden drop in hemoglobin. It is more common in children and is considered a medical emergency.
4. Hemolytic Crisis
During a hemolytic crisis, red blood cells break down faster than usual, causing worsening anemia. Patients may notice increasing fatigue, weakness, jaundice (yellowing of the eyes or skin), and dark-colored urine.
5. Acute Chest Syndrome
This is one of the most serious complications of sickle cell disease. It affects the lungs and may cause chest pain, fever, cough, breathing difficulty, and low oxygen levels. Urgent hospital treatment is required.
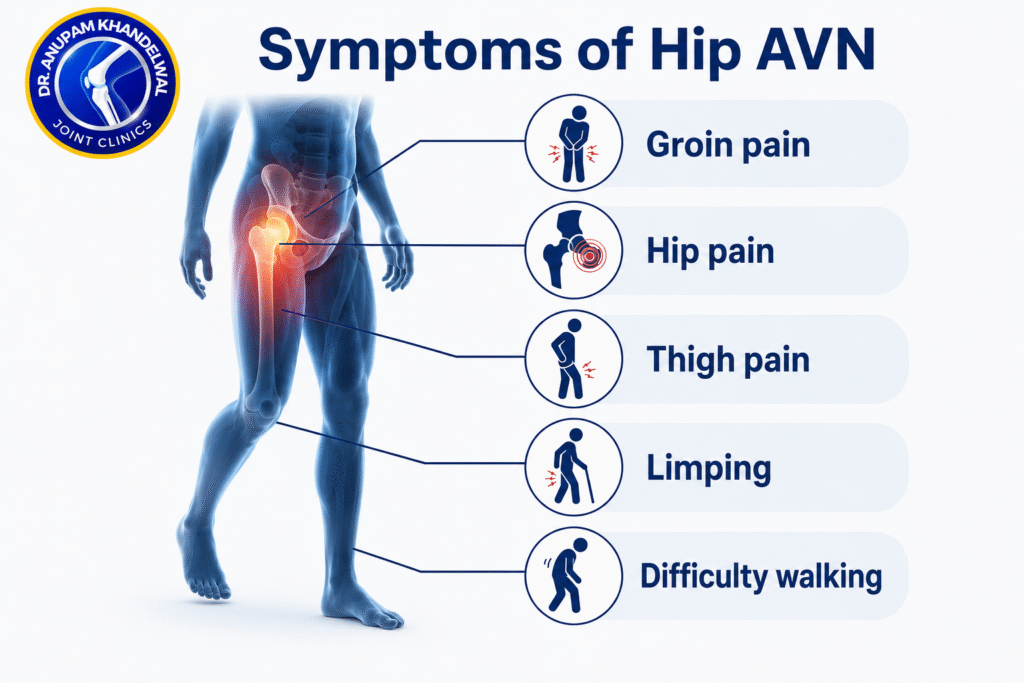
Symptoms of Avascular Necrosis in Sickle Cell
The symptoms usually develop gradually.
Common symptoms include:
- Deep pain in the groin
- Hip pain while walking
- Pain while climbing stairs
- Difficulty sitting cross-legged
- Limping
- Reduced hip movement
- Stiffness of the hip
- Pain that worsens with activity
- Difficulty standing for long periods
- Pain even during rest in advanced stages
Many patients initially assume these symptoms are simply another sickle cell pain crisis, delaying diagnosis.
Stages of Avascular Necrosis
Stage 1 – Early AVN
Stage 2 – Bone Damage Begins
Stage 3 – Bone Collapse
Stage 4 – Advanced Arthritis
How is Avascular Necrosis Diagnosed?
Early diagnosis greatly improves treatment outcomes.
Doctors may recommend:
Clinical Examination
The orthopedic surgeon checks:
- Hip movement
- Limp
- Pain location
- Walking pattern
X-ray
Useful in later stages but may appear normal during early AVN.
MRI Scan
MRI is the gold standard for diagnosing Avascular Necrosis in Sickle Cell because it detects bone damage before changes appear on X-rays.
CT Scan
Sometimes used to evaluate the amount of bone collapse before surgery.
Blood Tests
Blood investigations help assess:
- Severity of sickle cell disease
- Hemoglobin level
- Infection
- Other medical conditions
Explore our Sickle Cell Support Page to access trusted information, practical guidance, and detailed answers to frequently asked questions about living with sickle cell disease and preventing complications such as avascular necrosis.
Treatment of Avascular Necrosis in Sickle Cell
Treatment depends on:
- Stage of AVN
- Patient’s age
- Bone collapse
- Pain severity
- Daily activity level
Non-Surgical Treatment
1. Core Decompression
Core decompression is one of the most effective treatments for early AVN.
During surgery:
- Small channels are drilled into the affected bone.
- Pressure inside the bone decreases.
- Blood circulation improves.
- Healing is stimulated.
When performed before bone collapse, this procedure may delay or prevent hip replacement.
3. Stem Cell Therapy (Selected Patients)
Some orthopedic surgeons combine core decompression with bone marrow concentrate (BMAC) or stem cell therapy.
The concentrated bone marrow cells are injected into the affected bone to support healing.
Patient selection remains extremely important.
4. Bone Grafting
In certain patients, healthy bone grafts are used to support weakened bone and improve blood supplY
5. Total Hip Replacement
Once the femoral head collapses completely, hip replacement becomes the most reliable treatment.
Modern hip replacement provides:
- Excellent pain relief
- Better walking ability
- Improved quality of life
- Long-lasting implants
- Early return to daily activities
For many advanced cases of Avascular Necrosis in Sickle Cell, hip replacement offers the best long-term outcome.
Can AVN Be Prevented in Sickle Cell Disease?
Although AVN cannot always be prevented, its risk can be reduced by:
- Proper management of sickle cell disease
- Staying well hydrated
- Avoiding smoking
- Regular follow-up with a hematologist
- Early evaluation of persistent hip pain
- Prompt MRI when symptoms appear
- Maintaining a healthy lifestyle
- Avoiding unnecessary corticosteroid use
Early detection remains the key to preserving the hip joint.
Living with Avascular Necrosis in Sickle Cell
Receiving a diagnosis of AVN can be concerning, but many patients continue to lead active lives with timely treatment and proper medical care.
Successful management often involves a multidisciplinary approach that includes:
- Hematologist
- Orthopedic surgeon
- Physiotherapist
- Pain management specialist
- Rehabilitation team
Following medical advice, attending regular follow-ups, and reporting new symptoms early can significantly improve long-term outcomes.
FAQs
1. What is Avascular Necrosis in Sickle Cell Disease?
Avascular Necrosis (AVN) in Sickle Cell Disease is a condition in which reduced blood supply causes the bone tissue, most commonly the femoral head of the hip, to die. Repeated blockage of small blood vessels by sickle-shaped red blood cells increases the risk of bone damage and joint collapse.
2. Why are people with sickle cell disease at higher risk of AVN?
People with sickle cell disease have abnormal red blood cells that can block small blood vessels. These blockages reduce oxygen-rich blood flow to the bones, particularly the hip joint, making them more likely to develop Avascular Necrosis in Sickle Cell Disease.
3. What are the early symptoms of Avascular Necrosis in Sickle Cell Disease?
Early symptoms include persistent hip or groin pain, stiffness, pain while walking or climbing stairs, reduced range of motion, and limping. If these symptoms continue for more than a few weeks, an orthopedic evaluation is recommended.
4. How is Avascular Necrosis in Sickle Cell Disease diagnosed?
Diagnosis usually includes a physical examination, X-rays, and an MRI scan. MRI is the most sensitive test for detecting AVN in its early stages, even before changes become visible on X-rays.
5. Can Avascular Necrosis in Sickle Cell Disease be treated without surgery?
In the early stages, non-surgical treatments such as pain medication, activity modification, physiotherapy, and managing sickle cell disease may help relieve symptoms. However, these treatments cannot restore dead bone tissue, and surgery may be needed if the condition progresses.
6. What is the best treatment for Avascular Necrosis in Sickle Cell Disease?
The best treatment depends on the stage of the disease. Early-stage AVN may be treated with Core Decompression and, in selected patients, bone marrow concentrate (BMAC). Advanced stages with bone collapse often require Total Hip Replacement Surgery.
7.Who provides advanced treatment for Avascular Necrosis in Sickle Cell Disease in Indore?
Patients looking for advanced treatment for Avascular Necrosis in Sickle Cell Disease in Indore can consult Dr. Anupam Khandelwal, an Orthopaedic and Joint Replacement Surgeon with expertise in joint-preserving procedures, Core Decompression, and advanced Hip Replacement Surgery. Treatment is planned according to the stage of AVN, with the goal of relieving pain, preserving joint function whenever possible, and helping patients return to their daily activities.
About Dr. Anupam Khandelwal
Dr. Anupam Khandelwal is a renowned Orthopaedic and Joint Replacement Surgeon based in Indore, specializing in the treatment of hip and knee disorders, including Avascular Necrosis in Sickle Cell Disease. He has extensive experience in joint-preserving procedures such as Core Decompression and advanced Hip Replacement Surgery. Dr. Khandelwal focuses on early diagnosis, personalized treatment plans, and evidence-based orthopedic care to achieve the best possible outcomes. Patients from Indore, Madhya Pradesh, and across India trust him for advanced hip care and comprehensive rehabilitation aimed at restoring mobility and improving quality of life.
हिंदी सारांश
सिकल सेल रोग में असामान्य लाल रक्त कोशिकाएँ हड्डियों तक रक्त की आपूर्ति कम कर देती हैं, जिससे Avascular Necrosis (AVN) होने का खतरा बढ़ जाता है। इसका सबसे अधिक प्रभाव हिप (कूल्हे) के जोड़ पर पड़ता है। लगातार हिप या ग्रोइन में दर्द, चलने में कठिनाई और लंगड़ापन इसके शुरुआती संकेत हो सकते हैं। समय पर MRI जांच और ऑर्थोपेडिक विशेषज्ञ से उपचार कराने पर हिप जॉइंट को बचाने की संभावना बढ़ जाती है। शुरुआती अवस्था में Core Decompression और उन्नत अवस्था में Hip Replacement Surgery प्रभावी उपचार विकल्प हैं।
Muhtasari wa Kiswahili
Katika Sickle Cell Disease, chembe nyekundu za damu zenye umbo la mundu zinaweza kupunguza mtiririko wa damu kwenye mfupa wa nyonga na kusababisha Avascular Necrosis (AVN). Dalili za kawaida ni maumivu ya nyonga au kinena, ugumu wa kutembea, na kuchechemea. Uchunguzi wa mapema kwa kutumia MRI husaidia kugundua tatizo kabla mfupa haujaharibika sana. Matibabu ya mapema kama Core Decompression yanaweza kuhifadhi nyonga, huku Hip Replacement Surgery ikiwa chaguo bora kwa hatua za mwisho za ugonjwa.